- Research
- Open access
- Published:
The role of training and education for enhancing empathy among healthcare students: a systematic review of randomised controlled trials
BMC Medical Education volume 25, Article number: 469 (2025)
Abstract
Background
Empathy can lead to a better patient-professional relationship, and this skill that can be learned and trained, and the university is the ideal place to start this training. The aim of this systematic review is to assess whether training and education interventions have an impact on increasing empathy in health students.
Methods
The acronym PICOS was used to formulate the research question. A high-sensitivity search was made combining indexed terms, entry terms, and Boolean OR/AND in 9 databases, including grey literature and manual search of retrieved articles. Two researchers selected the studies based on previously established eligibility criteria. The risk of bias was verified using the RoB2 tool and a meta-analysis was performed using RevMan 5.4.
Results
The analysis included 30 studies in the qualitative synthesis and 20 studies that presented adequate data for the meta-analysis. An overall moderate effect on participants’ empathy was found after the intervention (standardized mean difference 0.45, 95% CI 0.25 to 0.65). However, heterogeneity was high (I2 = 79%). More than half of the studies were considered at high risk of bias. The results suggests that interventions can be effective in increasing empathy.
Conclusion
This topic has been in the spotlight in the area of health education in recent years. And more quality studies will be needed, as well as long-term evaluation of interventions to ensure the durability of empathy enhancement.
Clinical trial number
Not applicable.
Background
Empathy is a wide concept and plays an important role to all human connections every single day. The term that generated the word empathy in English is “Einfühlung”, a German word that appeared for the first time in the 19th century, more precisely in 1873, in Robert Vischer’s doctoral thesis. Empathy’s meaning has continually changed since the beginning of the 19th century. For psychologists, empathy is our ability to identify how someone else is feeling and respond to their feelings by understanding their emotions [1]. However, for philosophers’ empathy can be a response on how we can understand other people’s way of thinking [2] and more recently, according to phenomenologists empathy is the “other understanding”; they often mix the term empathy with other terms like “other-experience” and “other-perception” [3].
Empathy can also be described as a concept in between the cognitive and the affective domain. The cognitive domain stands for the ability of understanding someone’s feelings and still view from the outside of the other person’s perspective. The affective domain means that you understand and have the same feelings as the other person” [4, 5]. The American Medical Colleges Association once stated that medical schools should educate altruistic physicians on being compassionate and empathetic [6]. From the patient’s point of view, they tend to consider empathy a basic skill that can increase therapeutic relationship and treatment quality [7]. Frequently the terms empathy and sympathy are mixed, but in a patient-treatment situation they should be discerned. Empathy tends to emphasize the importance of sharing our understanding with a patient while sympathy emphasizes sharing our emotions. In this case, sympathy could even interfere with a patient’s diagnosis and treatment [8]. On the other hand, empathy should have no limits as it can always be advantageous in-patient care [9]. Clinical empathy can lead to a better patient-healthcare staff relationship [10] and is the center of humanistic healthcare [11] Empathy can be a learned skill [12]; that’s why medical or healthcare schools can be the suitable place to start preparing students skills in empathy [13]. For Costa-Drolon et al. [14], medical students are already a little troubled by all the theory regarding the concept of the term empathy. Empathy in a physicians should be seen as the seeking result not just a process [14].
On the other hand, several studies report that empathy levels decline as healthcare students’ progress through their training [15]. Recently Tariq et al. [16] declared that with formal activities throughout all clinical years we might help promote empathy in medical students. Several studies have already tried to fill in those gaps and reduce the decline of empathy. Education and training interventions can help to enhance empathy among healthcare staff mainly through undergraduate studies.
Several systematic reviews of enhancing empathy interventions have already been conducted, each one of them with different populations and methodologies. One of the first systematic reviews, Kelm et al. [17] focused on empathy changes for medical students, residents, fellows and physicians. Even though this systematic review supports the idea that interventions can increase empathy among medical students and physicians, most of the 64 included studies had a deficient research design, insufficient intervention information and scarce long-term evaluation. The systematic review made by Patel et al. [18] selected both randomized and observational studies and concluded that 75% of the studies verified that the tested curricula enhanced physicians’ empathy or compassion. They also pointed out the following behaviours that have a direct influence on improving the patient perception of empathy: sitting vs. standing while with a patient, detecting patient non-verbal cues, recognizing, and responding to signs of compassion, eye contact and verbal support. In 2020, Fragkos et al. [19] and Winter et al. [20] published systematic reviews that aimed to verify the effect of empathy-enhancing interventions in health education for healthcare students and professionals. They conclude that empathy interventions could be effective at promoting and maintaining empathy and that medical education is still under development.
Even though these previous systematic reviews confirmed empathy’s increase through education and training interventions [17,18,19,20] this subject requires additional investigation and a more rigorous methodology. For this reason, the present study aims to evaluate the role of education and training for promoting empathy among healthcare students.
Methods
This systematic review was developed in accordance with the Cochrane Handbook for Systematic Reviews of Interventions [21]. The search strategy and the definition of all entry and indexed terms were defined after the formulation of the research question PICOS (population, intervention, comparison, outcome and type of study), as described in Table 1 in supplement.
A preliminary search was conducted to verify the validity of the proposed subject. It was accomplished through PubMed and Cochrane, aiming to identify any previous existing systematic reviews. For this preliminary search, the following keywords were used: empathy, healthcare students, education and training. We also searched for potentially new relevant studies to guarantee there were enough new randomised controlled trials for conducting this systematic review. Additionally, we searched the Prospero registration platform to make sure there were no ongoing protocols with similar aims. These results justify the execution of the present study that may contribute and provide supplementary information about the importance of training and education interventions to increase healthcare students’ empathy.
This protocol was elaborated following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines’ latest version [22]. This systematic review protocol was registered with PROSPERO International prospective register of Systematic Reviews - (http://www.crd.york.ac.uk/PROSPERO/ - under the number CRD42023393608.
The PICOS acronym (Population, Intervention, Comparison, Outcome and Study type) was used to formulate the clinical question: Is there a difference in enhancing empathy (O) among healthcare students (P) from education and training intervention (I) over standard education (C) in randomised controlled trials (S)?
Our PICOS question was adopted as guidance to our research strategy, more details in supplement, Table 2 and 3. First, all indexed terms that could be used for an exhaustive search were verified, MeSH terms (Medical Subject Headings) - PubMed; DeCS terms – BVS; Entree terms – Embase. The final search strategy used a combination of all indexed terms and entry terms (synonyms). Boolean operators OR/AND were used to combine all indexed terms (MeSH, DeCS and Entree) and entry terms.
The exhaustive literature search was conducted throughout several electronic databases (PubMed, Cochrane Library, PsycINFO, EBSCO, Embase, Scopus, Web of Science, Science Direct and BVS), as well as a manual search through Google Scholar, OATD and a final search by hand-searching references of retrieved papers that could respond to our PICOS question. The full search strategy is available in Supplementary file, Tables 4, 5, 6, 7, 8, 9, 10, 11, 12, 13 and 14.
Only randomised controlled trials were selected, other kinds of studies were excluded. Systematic reviews with or without metanalysis were consulted for scientific concepts and methodological analysis, but they were not included in this study. All retrieved studies through this search strategy were stored using Mendeley Reference Manager, duplicates were removed, and all studies left were distributed to two investigators for studies selection.
Data extraction was executed by the two researchers independently (CTS and RTA) and there were no disagreements between them, so there was no need of consulting the third examiner (CR) for consensus. Studies that were excluded after eligibility were recorded in a ‘excluded studies’ table.
To evaluate de agreement between the authors, 10% of the publications was randomly chosen. They were compared to obtain the intra and inter-examiner Cohen Kappa’s coefficient. The PRISMA [22] flow diagram was used to record all process (screening and selection) and selected studies were fully read for data extraction. Information collected included author, year of publication, country of origin, number of participants, degree type, Intervention type, duration of intervention, outcome assessor, outcome measure, outcome assessment time and effect of intervention on empathy levels between groups (immediate post-test).
The risk of bias was assessed, for each included study, using the Cochrane Collaboration’s tool through the Cochrane risk-of-bias tool for randomized trials (RoB2). The RoB 2 evaluates five domains related to possible study biases [23].Each item was scored as low, some concerns or high risk of bias and evidence from the study were used to justify each score given and an overall risk of bias assessment of all included studies will be presented [23].
Quantitative data was collected and documented in an excel spreadsheet, eligibility criteria can be found in supplement, Table 15. To be included in the quantitative synthesis studies had to provide Mean and Standard Deviation from post-test from both intervention and control group. Results of post-test at follow-up were not considered as not all studies presented this data. Only studies with one intervention group and one control group were included.
Missing or unclear data for quantitative synthesis was requested by email directly to the corresponding author of the study.
After all data extraction, two subgroup analyses were conducted:
-
(1).
Degree of study: students from different degrees were analysed separately.
-
(2).
Outcome measure: different outcome measures were analysed separately (self and observer).
Data was inserted in the Software Rev.Man 5.4 (Review Manager 5.4) for the calculations and graphical presentation of the results through the forest Plots [24].
The random-effects model was used, since this model is the most recommended. As the studies under analysis form a random sample of a hypothetical population of studies. However, although the effects of the studies are not considered equal, they are related through a probability distribution, which is generally assumed to be normal [25].
Results
The literature search was performed from January 22nd2023 to March 28th2023 and retrieved 3701 records (3585 from databases and 116 from complementary searches). All 3701 records retrieved were stored using Mendeley Reference Manager, after removing duplicates, two researchers (CTS and RTA) proceeded verifying title/abstract and when needed the study was fully read, 38 studies were excluded as they were not fully retrieved, finally 168 studies were retrieved for eligibility. Among which, 30 studies were included in the qualitative synthesis. Figure 1 provides an overview of the selection process (PRISMA Flow Diagram). Characteristics of included studies are described in Figs. 2, 3 and 4. The list of all excluded studies and reason for exclusion described in Tables 16 and 17 in supplement.

PRISMA 2020 flow diagram selection process of included searches from databases and other sources
To verify the inter and intra-examiner’s reliability, 10% of the publications were randomly chosen. They were compared to obtain intra and inter-examiner Cohen Kappa’s coefficient, assessed through the IBM-SPSS Statistics (version 27). Tables 18 and 19 on supplemental materials show more details of each step verified and results. Values of Kappa above 0.9 are considered as an almost perfect level of agreement and have 82–100% of reliable data [26].
A total of 30 randomised controlled trials were analysed with a total number of 3486 healthcare students. It is not possible to know exactly how many female students were and how many were male students as three studies did not mention this data [27,28,29]. All included studies were conducted with healthcare students from four different degree types (three with pharmacy students [30,31,32], thirteen with medical students [27,28,29, 33,34,35,36,37,38,39,40,41,42], thirteen with nursing students [43,44,45,46,47,48,49,50,51,52,53,54] and nursing/midwifery [55]. There was no randomised controlled trial with dentistry students.
The studies were conducted in fifteen different countries, eleven studies came from Asia (four from China [42, 52, 53, 56], two from Turkey [43, 47], one from Thailand [36], one from India [37], two from Iran [49, 51] and one from Malaysia [57] ), ten studies from North America (nine from the USA [29,30,31, 35, 38, 39, 41, 44, 50] and one from Canada [28]), seven studies from Europe (two from Spain [45, 46], two from France [33, 34], one from Germany [27], one in Italy [48] and one in the United Kingdom [54]), one study from Australia/Oceania (New Zealand) [40] and one study from Africa(Ghana) [55]. Study publication dates ranged from 1987 to 2023, eighteen studies were published in the last five years [32, 33, 37, 39, 42,43,44,45,46,47,48,49, 51,52,53,54,55,56].
Studies sample size ranged from 21 to 362 participating students, fourteen studies had more than 100 participants [27, 28, 32,33,34,35, 42, 43, 46, 48, 52,53,54,55], thirteen studies had between 50 and 100 participants [29, 35, 36, 38, 40, 41, 44, 45, 47, 49,50,51, 56] and only three studies had less than 50 participants [30, 31, 39].
Studies were conducted with healthcare students through different types of interventions such as: communications/empathy skills training [27,28,29, 37, 38, 44, 46, 49, 55]; mindfulness training [41, 43]; narrative/literature intervention [30, 33, 53, 56]; simulation intervention [32, 35, 45, 50, 52]; role play technique [31, 36, 51]; transformative learning theory [47]; patient-experience training [48]; video or digital intervention [39, 52]; empathy intervention/innovation [40, 42] and Balint groups [30, 31].
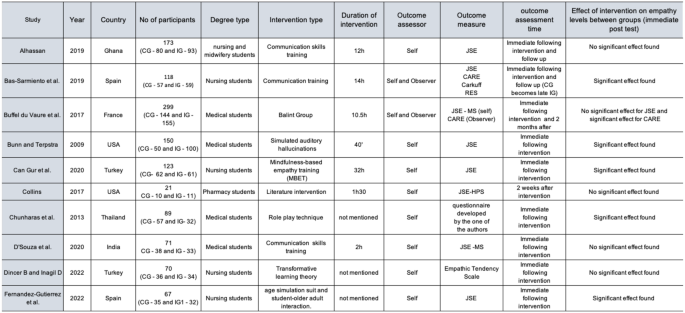
Characteristics of all included studies
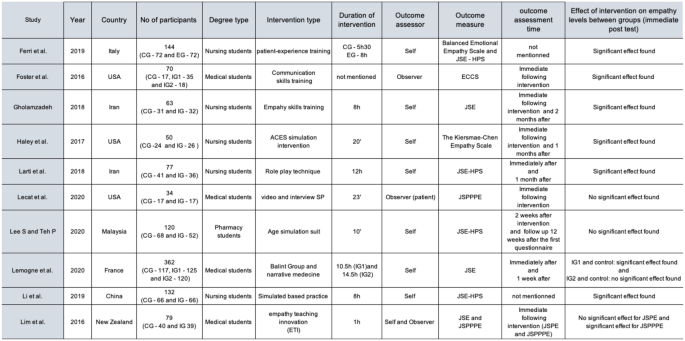
Characteristics of all included studies. Source: The authors
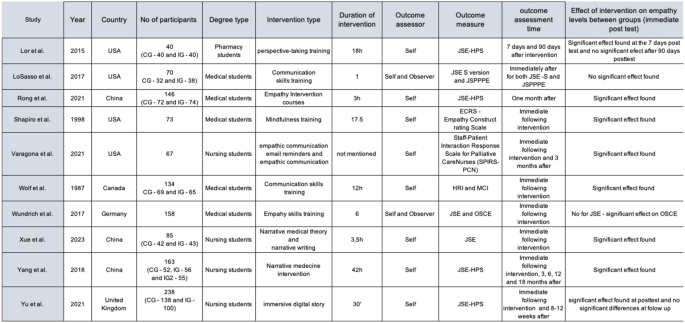
Characteristics of all included studies. Source: The authors
The Cochrane risk-of-bias tool for randomized trials (RoB2) was used to assess the risk of bias [17]. The RoB2 evaluates five domains related to possible study biases (randomisation process, deviation from the intended intervention, missing outcome data, measurement of the outcome and selection of the reported results).
Each study was evaluated for each of these domains and scored as low, some concerns or high risk of bias and evidence from the study was used to justify each score given. The overall risk of bias can be found at Fig. 5.

Overall Risk of bias assessment the RoB2 tool
Studies were considered at low risk of bias if all domains were judged as been at low risk, some concerns if a few domains are judged as some concern and high risk of bias if at least one outcome domain was judged at high risk or multiple domains judged to be of some concern [17]. Among 30 studies, eighteen were considered high risk of bias [24,25,26, 28, 32, 33, 38, 40, 42,43,44,45,46, 48, 50, 52], eleven were considered with some concerns [27, 31, 34,35,36,37, 39, 47, 49, 51, 53] and one was considered as low risk of bias [29]. See supplement Tables 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48 and 49 for Risk of Bias of all included studies and support for judgement.
Meta-analysis results
Of the 30 studies included in this systematic review, 10 studies were excluded from the meta-analysis. Seven of them were excluded after the primary analysis, as they did not provide adequate data (Mean and SD) from which to calculate the Standardized mean difference (SMD). Two of those studies provided only percentage data [33, 36], two studies provided only median information [39, 44] and three studies did not provide any data [24, 38, 41]. Missing or unclear data for the meta-analysis was requested by email directly to all corresponding authors. Only two authors [33, 41] returned our emails and could not provide the requested data.
The other 3 studies [30, 35, 50] were excluded since they had two intervention groups and one control group, considering that an inclusion criteria for the meta-analysis was only studies with one intervention and one control group. At the end 20 studies were included in the meta-analysis.
The primary analysis presents the results of the meta-analysis for all included studies concerning healthcare students (Fig. 6). The figure shows: the forest plot, the statistical measures of the studies (mean, standard deviation and n for intervention and control groups), study weight, standard mean difference, the respective 95% confidence interval, as well as the results of the test Cochran’s Q, the value of the I2 statistics. One study [37] was not included in this overall meta-analysis as it provided only observer assessor data (through JSPPPE) and all the other studies were self-assessor (through JSE). One study [43] was included separately as centre 1 and centre 2 as the data provided by the authors already separated both centres.
Analysing the results presented (Fig. 6), regarding the 95% confidence interval associated with the difference in means, the studies: Alhassan, 2019; Bas-Sarmiento et al., 2019; Bunn and Terpstra, 2009; Collins et al., 2017; D’Souza et al., 2020; Lee and Teh, 2020 and LoSasso et al., 2017 contain the value zero, so it can be inferred that the differences between the experimental group and the control group are not statistically significant. On the other hand, it is observed that the studies: Bas-Sarmiento et al., 2019 (center2); Lee and Teh, 2020 and Wolf et al., 1987, present a treatment effect that favours the control group, because they are to the left of the vertical line, whilst the other studies favours the experimental group.
The forest plot shows a total of 1122 participants on the intervention group and 1037 participants on the control group and an overall moderate effect on participants empathy postintervention favouring the experimental group (SMD 0.45, 95% CI 0.25 to 0.65). This influence is statistically significant which is further confirmed by the statistic Z = 4.43 with p < 0.001.
As for heterogeneity, Cochran’s Q (p < 0.001) and I2 = 79% are observed, suggesting a high heterogeneity.

Meta-analysis results for all healthcare students
Sensitivity analysis
Due to the high heterogeneity (I2 = 79%), it was decided to explore this heterogeneity by conducting a sensitivity analysis. The sensitivity analyses were managed by assessing the risk of bias of each study. The studies that were judged as high risk of bias were excluded from this new forest plot (Fig. 7).

Meta-analysis results for all healthcare students without high-risk of bias studies
The new forest plot (Fig. 7) shows a total of 484 participants on the intervention group and 489 participants on the control group and an overall moderate effect on participants empathy postintervention favoring the experimental group (SMD 0.45, 95% CI 0.20 to 0.70). This influence is statistically significant which is further confirmed by the statistic Z = 3.52 with p < 0.001 and I2 = 69% remained considerable, although the intensity decreased.
Participant population subgroup analysis
The overall Effect (Fig. 8) on participants empathy postintervention favours the experimental group (standardized mean difference 0.45, 95% CI 0.25 to 0.65). This influence is statistically significant. However, due to the high heterogeneity (I2 = 79%), It was decided to explore de heterogeneity by conducting a subgroup meta-analysis31 and try to examine potential sources of heterogeneity in our overall meta-analysis, and, if possible, to identify where heterogeneity came from. First, analysing the results of test for subgroup differences, it shows that the subgroups appear to have different effects (p = 0.05).

Meta-analysis subgroup results participant population
The subgroup medical students shows a total of 391 participants on the intervention group and 333 participants on the control group and a not statistically significant effect on participants empathy postintervention (SMD 0.11, 95% CI -0.25 to 0.46), I2 = 80%, suggesting a high heterogeneity between studies.
The subgroup pharmacy students shows a total of 83 participants on the intervention group and 98 participants on the control group and a not statistically significant effect on participants empathy postintervention (SMD 0.30, 95% CI -0.25 to 0.84), I2 = 60%, suggesting a moderate heterogeneity between studies from this subgroup.
The subgroup nursing students shows a total of 648 participants on the intervention group and 606 participants on the control group and moderate effect on participants empathy postintervention favouring the experimental group (SMD 0.63, 95% CI 0.39 to 0.87), I2 = 76%, suggesting a high heterogeneity between studies from this subgroup.
The medical students and the nursing students subgroups have a high heterogeneity (respectively 80% and 76%) and the pharmacy students subgroup a moderate heterogeneity (60%), which can imply that the heterogeneity might not only depend on the degree being analysed (because subgroups have different effects) but also another aspect within those subgroups, mainly for medical and nursing students.
This heterogeneity can be due to clinical or methodological differences and different kinds of interventions used by these studies, but to be sure we would have to make new subgroups from each subgroup.
Outcome assessor analysis – self-assessed
Figure 6 shows a total of 1001 participants on the intervention group and 944 participants on the control group and an overall moderate effect on participants empathy postintervention favouring the experimental group (SMD 0.45, 95% CI 0.29 to 0.60). This influence is statistically significant which is further confirmed by the statistic with p < 0.001.
As for heterogeneity, Cochran’s Q (p < 0.001) and I2 = 69% are observed, suggesting a moderate heterogeneity.
When analysing the results of test for subgroup differences, it shows that the subgroups appears to have similar effects (p = 0.14), Fig. 9.

Meta-analysis Subgroup results self-assessed
The subgroup JSE-S version shows a total of 326 participants on the intervention group and 264 participants on the control group and a statistically significant effect on participants empathy postintervention (SMD 0.31, 95% CI 0.14 to 0.47), I2 = 0%, suggesting a low heterogeneity between studies.
The JSE-HPS version shows a total of 675 participants on the intervention group and 680 participants on the control group and a statistically significant effect on participants empathy postintervention (SMD 0.50, 95% CI -0.30 to 0.71), I2 = 69%, suggesting a substantial heterogeneity between studies from this subgroup.
We can conclude that the heterogeneity is not due to the kind of instrument (JSE-S version or HPS-version) but to another source within the studies of the JSE-HPS subgroup.
Outcome assessor analysis – Observer-assessed.
Figure 10 shows a total of 291 participants on the intervention group and 273 participants on the control group and a not statistically significant effect on participants empathy postintervention favouring the control group (SMD 0.29, 95% CI -0.050 to 0.63), p = 0.10. As for heterogeneity, Cochran’s Q (p < 0.001) and I2 = 69% are observed, suggesting a moderate heterogeneity [30]. Analysing the results of test for subgroup differences, it shows there is evidence that the effect is different in the subgroups (p = 0.02), meaning that there are differences between the CARE and the JSPPPE.
The CARE subgroup presents a statistically significant effect on participants empathy postintervention favouring the experimental group, while the JSPPPE presents a non-statistically.
significant effect on participants empathy postintervention favouring the control group.
Also, when looking the heterogeneity, only the CARE subgroup has a substantial heterogeneity (I2 = 66%) which suggests there is an aspect causing the heterogeneity which does not depend on the studies of the JSPPPE subgroup.

Meta-analysis Subgroup results observer-assessed
The certainty of evidence was performed using GRADE pro, (Fig. 11), the quality of evidence is very low due to serious risk of bias (twelve studies included were considered high risk and seven had uncertainty risk of bias) and very serious inconsistency (high heterogeneity between studies − 79%).

GRADE tool analysis
Discussion
Enhancing healthcare students’ and personnel’s empathy has been a constant area of interest in health education. The empathetic ability of both undergraduate students and professionals is the primary step to achieve better patients’ outcomes, through a closer relationship between patient-healthcare providers and increasing treatment adherence. Even though in the last few years several studies were published, there are still a few questions that remain unanswered. Also, universities and health educators should join forces to develop empathy in health curricula.
There are a few previous systematic reviews confirming empathy’s increase through education and training interventions [21,22,23,24,25, 58,59,60] but this subject required additional investigation due to several new studies that have been published since then. The main aim of this systematic review was to evaluate the role of education and training for promoting empathy among healthcare students. Through this systematic review, training and education were validated as ways of increasing empathy, as the results of 17 studies show a significant impact. Also, the meta-analysis showed as overall moderate effect favouring the experimental group.
Previous systematic reviews had as an inclusion criteria only English studies; however, as this can lead to publication bias, in systematic review we aimed to reduce this bias choosing to have no restriction regarding the language of publication. We also decided not to have any restrictions regarding the time of publication and used more databases than all the other systematic reviews and included a complementary search at Google Scholar and OATD.
To our knowledge, this was the first systematic review and meta-analysis of randomised controlled trials performed only with healthcare students, without any language and time of publication restriction. There are 8 previous systematic reviews, of which, two studies verified empathy changes on students but without mixing different degrees (only nursing students [58] and only medical students [24]), two selected only health professionals [22, 23], two studies selected multiple types of participants [21, 25] (students and professionals), and the last two reviews [59, 60], aimed to study the effectiveness of interventions in healthcare students, but both studies limited their research on simulation-based interventions and they did not stipulate a study design.
Of the 30 included studies, 26 studies were with nursing and medical students; these two degrees are known for showing a significant enhancement in empathy compared to others. Even though our review could find studies with other degrees (pharmacy [41, 50, 53] and midwifery [3]) there were several courses that were not represented in this review (dentistry, physiotherapy, occupational therapy) as they were no randomised controlled trials published. This shows the importance of conducting new trials with other healthcare students aiming to provide a more trustworthy result.
The included studies came from 5 different continents: Asia [26, 40, 42, 43, 46, 48, 50, 51, 55, 61, 62], North America [28, 39, 41, 45, 47, 49, 53, 54, 56, 57]), Europe [27, 29, 37, 38, 44, 63, 64], Australia/Oceania [52] and Africa [36]. It was possible to notice an increased effect on empathy in studies from Europe, North America and Asia. This increase can be explained due to cultural habits. For Lorié et al., there are still gaps that need to be accessed and more training programs with patients from different backgrounds are needed [65].
Even if there is a common belief that women are more empathetic than men evidence shows that men and women may experience and express empathy differently, although these differences can vary widely among individuals. Generally, studies indicate that women tend to score higher on measures of emotional empathy, which involves the ability to feel and share the emotions of others. They may be more attuned to nonverbal cues and emotional expressions, leading to a deeper emotional connection in social situations.
On the other hand, men may exhibit more cognitive empathy, which involves understanding another person’s perspective or feelings without necessarily sharing those emotions. This can sometimes manifest as a more analytical approach to empathy, focusing on problem-solving rather than emotional engagement. We could not verify this throughout our review as not all studies provided information about the sex/gender of participants and even fewer studies provided post-test results linked with this information to state if empathy was higher in women than in men. Future studies should try to provide empathy post-test results divided by sex/gender to make the comparison between women and men possible.
Another important point that should be highlighted is that although the JSE questionnaire is already validated in several languages and is widely used and known as an empathy measurement instrument, there is not a consensus, as there are still recent studies that used other outcome-measure instruments. Twenty [26, 27, 29, 36,37,38,39, 41, 42, 44, 46, 48, 50, 51, 53, 57, 61,62,63,64] studies used the JSE, three [49, 52, 54] studies used the and the JSPPPE and two studies used the CARE [37, 38] questionnaire. Training and education interventions had a significant impact on increasing empathy in 17 studies; in the others, the increase was considered non-existent or variable according to the questionnaire used.
Those results are aligned with other systematic reviews, that had also different results from the same study according to the type of instrument that was used [21, 24, 25, 59].
As stated by Fragkos et al. [24] self-reported instruments can be biased if we consider that students can feel compelled to answer in a certain way to avoid being criticized. For Salters-Pedneault [66] this can be considered a desirability bias, meaning that students can be inclined to give an answer aiming to increase their empathy scores. On the other hand, an observer-rate instrument, like the JSPPPE, can be assessed by simulated patients, university personnel, or independent observers and could help to remove desirability bias. However, our review had only a few studies that chose to evaluate students through observer instruments. This was also described by previous reviews [24, 25, 58,59,60], researchers might find it laborious and more expensive to have a third person dedicated only to observe and rate students after the intervention.
We decided to perform a meta-analysis and after data extraction (Mean and SD), twenty studies [26, 29, 36,37,38,39, 41, 42, 44, 46,47,48, 50,51,52,53,54, 57, 61, 63] were included. Even though heterogeneity was high, there was an overall moderate effect on participants’ empathy postintervention favouring the experimental group. Those findings were also noticed by previous reviews [24, 25, 59, 60]. We performed a sensitivity analyses to explore heterogeneity, and all high-risk of bias studies were removed, which maintained an overall moderate effect on participants empathy postintervention favouring the experimental group, but did not reduce the heterogeneity only decreasing its intensity.
This was the first systematic review with meta-analysis to explore heterogeneity. Previous systematic reviews also performed subgroup meta-analysis but never tried to identify its source.
Even if some studies presented follow-up data, we chose not to include this in our meta-analysis like another previous study [25]. We had a reason not to do so: first, there were several follow-up periods used by some studies. Also, two studies [36, 37] did their follow-up after their control group became a delayed intervention group, which did not seem suitable. Three previous systematic reviews [58,59,60] also addressed this lack of follow-up.
We also decided not to present the data dividing the various types of interventions, the great variety and mixed terminology of each intervention did not seem adequate at the time, but this decision might have been our weakness. Exploring this data might have helped us to understand the meta-analysis heterogeneity of some subgroups.
We had a few limitations to our study, the first of them being the risk of bias tool used. Normally for randomised controlled trials the chosen tool is RoB2, but we realized that due to the design of empathy studies, several studies were rated as being high-risk bias. The first main point that raised problems was that empathy education interventions cannot be blinded neither to the instructor nor to the students. The second was that the main instrument to measure students’ empathy is self-assessed (JSE). The JSE is validated in several countries worldwide and is the most used instrument by studies, but as it is self-observed, it tends to be considered high-risk at this domain. It seems that there should be a modified RoB2 to not overlook some types of study designs as those included in this systematic review.
Another limitation was a lack of long-term follow-up assessments. Unfortunately, without these assessments it is impossible to predict the students’ abilities to employ their new acquired empathy training to clinical practice.
Our last limitations were due to the meta-analysis. The first one was the diverse number of different interventions and our lack of prediction to verify each type of intervention separately. The second was substantial heterogeneity results: even if we aimed to predict the source of the heterogeneity, by pursuing a subgroup meta-analysis, more analysis would have been needed to answer this question and for some subgroups, even this extra analysis would not have been possible as the statistical strength weakens after several subgroups group analysis. Thirdly, it is also suggested that all subgroups analysis are predicted before the study, which was impossible to do as we only had the final information after the first analysis [30].
The findings of our systematic review can provide a solid foundation and guide health educators to design new curricular programs aiming the promotion of empathy and researchers by addressing gaps that should be verified while developing new studies.
Educators should try to foster a classroom and clinical environment where students feel safe to express their emotions and discuss challenges related to empathy and patient care as well as encouraging self-reflection such as journaling or group discussions, helping students to evaluate their experiences and feelings regarding patient interactions and empathy development.
Also develop peer mentorship programs where students can support each other and share experiences related to empathy in clinical settings and receive regular feedbacks.
Researchers should try to create new assessment tools that capture the multidimensional aspects of empathy, including self-report measures, peer assessments, and observational evaluations in clinical settings as well as combining quantitative and qualitative research methods to gain a deeper understanding of empathy by incorporating interviews, focus groups, and reflective essays alongside traditional surveys.
More quality studies will be needed, with long duration and long-term evaluation of interventions (follow-up) that follow students through their training and into practice to assess how empathy evolves and what factors influence these changes.
Conclusion
This topic has been in the spotlight in health education in recent years and will continue to be researched. We could conclude that:
-
Education and training interventions have a positive impact on students’ empathy scores; enhancing empathy through education is essential for fostering compassionate and patient-centered care in clinical practice.
-
Integrating empathy training into healthcare curricula can equip future professionals with the skills to connect with patients on a deeper level, thereby improving communication, trust, and overall patient satisfaction.
-
By prioritizing empathy in healthcare education, we can better prepare students to address the emotional and social complexities of patient care, leading to improved health outcomes and a more humane healthcare system.
-
The metanalysis results show an overall moderate effect on participants empathy postintervention favoring the experimental group;
-
It is extremely necessary to include students from other healthcare disciplines, other than medical, nursing and pharmacy aiming to achieve reliable results in between all healthcare fields;
-
The limitations we encountered may have influenced the interpretation of the results as it is difficult to evaluate different outcome assessors as they can influence the results.
-
The lack of long-term follow-up might have limited our capability to understand the real impact of healthcare interventions, researchers should also try to design new trials with ongoing assessments and long-term evaluations of empathy enhancement interventions;
-
Although randomised controlled trials are are considered the gold standard in clinical research for evaluating the efficacy of interventions, we encountered a problem when evaluating empathy interventions as they can not be blinded, and this impacts directly the the risk of bias of all studies.
Data availability
All data generated or analysed during this study are included in this published article.
Abbreviations
- CARE:
-
Consultation and relational empathy
- ECCS:
-
Empathic Communication Coding System
- ECRS:
-
Empathy Construct rating Scale
- HP-version:
-
Health professionals’ version
- HPS-version:
-
Health professions students
- JSE:
-
Jefferson Scale of Empathy
- JSPPPE:
-
Jefferson Scale of Patient Perceptions of Physician Empathy
- MeSH:
-
Medical Subject Headings
- OATD:
-
Open Access Theses and Dissertations
- PICO:
-
Population, Intervention, Comparison Outcome
- PICOS:
-
Population, Intervention, Comparison Outcome, Study type
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- Rev.Man 5.4:
-
Review Manager 5.4
- RoB2:
-
Cochrane risk-of-bias tool for randomized trials
- SD:
-
Standard Deviation
- SMD:
-
Standardized mean difference
- S-version:
-
Medical students version
References
Pearce S. Zero Degrees of Empathy: A New Theory of Human Cruelty By Simon Baron-Cohen. Allen Lane Publishing. 2011. £20.00 (hb). 208pp. ISBN: 9780713997910. British Journal of Psychiatry 2011;199:520–520. https://doiorg.publicaciones.saludcastillayleon.es/10.1192/bjp.bp.111.098434
Shanton K, Goldman A, Simulation. theory. WIREs Cognitive Science 2010;1:527–38. https://doiorg.publicaciones.saludcastillayleon.es/10.1002/wcs.33
Scheler M, McAleer G. The nature of sympathy. Routledge; 2017. https://doiorg.publicaciones.saludcastillayleon.es/10.4324/9781315133348.
Hojat M, Mangione S, Gonnella JS, Nasca T, Veloski JJ, Kane G. Empathy in medical education and patient care. Acad Med. 2001;76:669. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/00001888-200107000-00001.
Aring CD. SYMPATHY AND EMPATHY. J Am Med Assoc. 1958;167:448. https://doiorg.publicaciones.saludcastillayleon.es/10.1001/jama.1958.02990210034008.
Learning Objectives for Medical Student Education— Guidelines for Medical Schools. Report I of the medical school objectives project. J Association Am Med Colleges. 1999;74:13–8. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/00001888-199901000-00010.
Derksen F, Bensing J, Lagro-Janssen A. Effectiveness of empathy in general practice: a systematic review. Br J Gen Pract. 2013;63:e76–84. https://doiorg.publicaciones.saludcastillayleon.es/10.3399/bjgp13X660814.
Nightingale SD, Yarnold PR, Greenberg MS. Sympathy, empathy, and physician resource utilization. J Gen Intern Med. 1991;6:420–3.
Hojat M, Gonnella JS, Nasca TJ, Mangione S, Vergare M, Magee M. Physician empathy: definition, components, measurement, and relationship to gender and specialty. Am J Psychiatry. 2002;159:1563–9. https://doiorg.publicaciones.saludcastillayleon.es/10.1176/appi.ajp.159.9.1563.
Riess H, Kelley JM, Bailey RW, Dunn EJ, Phillips M. Empathy training for resident physicians: A randomized controlled trial of a Neuroscience-Informed curriculum. J Gen Intern Med. 2012;27:1280–6. https://doiorg.publicaciones.saludcastillayleon.es/10.1007/s11606-012-2063-z.
Veloski JJ. Mohammadreza Hojat. Measuring Medical Professionalism. New York: 2006.
Alligood MR, EMPATHY:, THE IMPORTANCE OF RECOGNIZING TWO TYPES. J Psychosoc Nurs Ment Health Serv. 1992;30:14–7. https://doiorg.publicaciones.saludcastillayleon.es/10.3928/0279-3695-19920301-06.
Ren GSG, Min JTY, Ping YS, Shing LS, Win MTM, Chuan HS, et al. Complex and novel determinants of empathy change in medical students. Korean J Med Educ. 2016;28:67–78. https://doiorg.publicaciones.saludcastillayleon.es/10.3946/kjme.2016.11.
Costa-Drolon E, Verneuil L, Manolios E, Revah-Levy A, Sibeoni J. Medical students’ perspectives on empathy: A systematic review and metasynthesis. Acad Med. 2021;96:142–54. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/ACM.0000000000003655.
Neumann M, Edelhäuser F, Tauschel D, Fischer MR, Wirtz M, Woopen C, et al. Empathy decline and its reasons: A systematic review of studies with medical students and residents. Acad Med. 2011;86:996–1009. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/ACM.0b013e318221e615.
Enhancing Empathy in Medical Students by Focused Learner Centered Activities. J Coll Physicians Surg Pakistan. 2023;33:79–83. https://doiorg.publicaciones.saludcastillayleon.es/10.29271/jcpsp.2023.01.79.
Kelm Z, Womer J, Walter JK, Feudtner C. Interventions to cultivate physician empathy: a systematic review. BMC Med Educ. 2014;14:219. https://doiorg.publicaciones.saludcastillayleon.es/10.1186/1472-6920-14-219.
Patel S, Pelletier-Bui A, Smith S, Roberts MB, Kilgannon H, Trzeciak S, et al. Curricula for empathy and compassion training in medical education: A systematic review. PLoS ONE. 2019;14:e0221412. https://doiorg.publicaciones.saludcastillayleon.es/10.1371/journal.pone.0221412.
Fragkos KC, Crampton PES. The effectiveness of teaching clinical empathy to medical students: A systematic review and Meta-Analysis of randomized controlled trials. Acad Med. 2020;95:947–57. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/ACM.0000000000003058.
Winter R, Issa E, Roberts N, Norman RI, Howick J. Assessing the effect of empathy-enhancing interventions in health education and training: a systematic review of randomised controlled trials. BMJ Open. 2020;10:e036471. https://doiorg.publicaciones.saludcastillayleon.es/10.1136/bmjopen-2019-036471.
Book Series C, Higgins JP, Green S. Cochrane Handbook for Systematic Reviews of Interventions THE COCHRANE COLLABORATION ®. n.d.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;n71. https://doiorg.publicaciones.saludcastillayleon.es/10.1136/bmj.n71.
Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;l4898. https://doiorg.publicaciones.saludcastillayleon.es/10.1136/bmj.l4898.
Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. Introduction to Meta-Analysis. Wiley; 2009. https://doiorg.publicaciones.saludcastillayleon.es/10.1002/9780470743386.
Rodrigues CL, Klarmann Ziegelmann P. Seção de bioestatística metanálise: um guia prático meta-analysis: a practical guide. vol. 30. 2010.
McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22:276–82.
Wündrich M, Schwartz C, Feige B, Lemper D, Nissen C, Voderholzer U. Empathy training in medical students – a randomized controlled trial. Med Teach. 2017;39:1096–8. https://doiorg.publicaciones.saludcastillayleon.es/10.1080/0142159X.2017.1355451
Wolf FM, Woolliscroft JO, Calhoun JG, Boxer GJ. A controlled experiment in teaching students to respond to patientsʼ emotional concerns. Acad Med. 1987;62:25–34. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/00001888-198701000-00004.
LoSasso AA, Lamberton CE, Sammon M, Berg KT, Caruso JW, Cass J, et al. Enhancing student empathetic engagement, History-Taking, and communication skills during electronic medical record use in patient care. Acad Med. 2017;92:1022–7. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/ACM.0000000000001476.
Collins KL, Zweber A, Irwin AN. Impact of a fictional reading intervention on empathy development in student pharmacists. Curr Pharm Teach Learn. 2017;9:498–503. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.cptl.2016.12.003.
Lor KB, Truong JT, Ip EJ, Barnett MJ. A randomized prospective study on outcomes of an empathy intervention among second-year student pharmacists. Am J Pharm Educ. 2015;79:18. https://doiorg.publicaciones.saludcastillayleon.es/10.5688/ajpe79218.
Lee SWH, Teh P-L. Suiting up to enhance empathy toward aging: A randomized controlled study. Front Public Health. 2020;8. https://doiorg.publicaciones.saludcastillayleon.es/10.3389/fpubh.2020.00376.
Lemogne C, Buffel du Vaure C, Hoertel N, Catu-Pinault A, Limosin F, Ghasarossian C, et al. Balint groups and narrative medicine compared to a control condition in promoting students’ empathy. BMC Med Educ. 2020;20:412. https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12909-020-02316-w.
Buffel du Vaure C, Lemogne C, Bunge L, Catu-Pinault A, Hoertel N, Ghasarossian C, et al. Promoting empathy among medical students: A two-site randomized controlled study. J Psychosom Res. 2017;103:102–7. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.jpsychores.2017.10.008.
Bunn W, Terpstra J. Cultivating empathy for the mentally ill using simulated auditory hallucinations. Acad Psychiatry. 2009;33:457–60. https://doiorg.publicaciones.saludcastillayleon.es/10.1176/appi.ap.33.6.457.
Chunharas A, Hetrakul P, Boonyobol R, Udomkitti T, Tassanapitikul T, Wattanasirichaigoon D. Medical students themselves as surrogate patients increased satisfaction, confidence, and performance in practicing injection skill. Med Teach. 2013;35:308–13. https://doiorg.publicaciones.saludcastillayleon.es/10.3109/0142159X.2012.746453.
D’souza PC, Rasquinha SL, D’souza TL, Jain A, Kulkarni V, Pai K. Effect of a Single-Session communication skills training on empathy in medical students. Acad Psychiatry. 2020;44:289–94. https://doiorg.publicaciones.saludcastillayleon.es/10.1007/s40596-019-01158-z.
Foster A, Chaudhary N, Kim T, Waller JL, Wong J, Borish M, et al. Using virtual patients to teach empathy. Simul Healthcare: J Soc Simul Healthc. 2016;11:181–9. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/SIH.0000000000000142.
Lecat P, Dhawan N, Hartung PJ, Gerzina H, Larson R, Konen-Butler C. Improving patient experience by teaching empathic touch and eye gaze: A randomized controlled trial of medical students. J Patient Exp. 2020;7:1260–70. https://doiorg.publicaciones.saludcastillayleon.es/10.1177/2374373520916323.
Lim BT, Moriarty H, Huthwaite M, Gallagher P, Perera R. Teaching empathy to undergraduate medical students: translation to practice. Focus Health Prof Education: Multi-Professional J. 2016;17:59. https://doiorg.publicaciones.saludcastillayleon.es/10.11157/fohpe.v17i1.122.
Shapiro SL, Schwartz GE, Bonner G. Effects of mindfulness-based stress reduction on medical and premedical students. J Behav Med. 1998;21:581–99. https://doiorg.publicaciones.saludcastillayleon.es/10.1023/A:1018700829825.
Rong R, Chen W, Dai Z, Gu J, Chen W, Zhou Y, et al. Improvement of the management of mental well-being and empathy in Chinese medical students: a randomized controlled study. BMC Med Educ. 2021;21:378. https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12909-021-02813-6.
Can Gür G, Yilmaz E. The effects of mindfulness-based empathy training on empathy and aged discrimination in nursing students: A randomised controlled trial. Complement Ther Clin Pract. 2020;39:101140. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.ctcp.2020.101140.
Varagona L, Myers R, Wilson A. Weekly email reminders increase nursing students’ use of empathic communication. Nurse Educ. 2021;46:366–71. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/NNE.0000000000000978.
Fernández-Gutiérrez M, Bas-Sarmiento P, del Pino-Chinchilla H, Poza-Méndez M, Marín-Paz AJ. Effectiveness of a multimodal intervention and the simulation flow to improve empathy and attitudes towards older adults in nursing students: A crossover randomised controlled trial. Nurse Educ Pract. 2022;64:103430. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.nepr.2022.103430.
Bas-Sarmiento P, Fernández-Gutiérrez M, Díaz-Rodríguez M, Carnicer-Fuentes C, Castro-Yuste C, García-Cabanillas MJ, et al. Teaching empathy to nursing students: A randomised controlled trial. Nurse Educ Today. 2019;80:40–51. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.nedt.2019.06.002.
Dincer B, Inangil D. The effect of affective learning on alexithymia, empathy, and attitude toward disabled persons in nursing students: A randomized controlled study. Perspect Psychiatr Care. 2022;58:813–21. https://doiorg.publicaciones.saludcastillayleon.es/10.1111/ppc.12854.
Ferri P, Rovesti S, Padula MS, D’Amico R, Di Lorenzo R. Effect of expert-patient teaching on empathy in nursing students: a randomized controlled trial. Psychol Res Behav Manag 2019;Volume 12:457–67. https://doiorg.publicaciones.saludcastillayleon.es/10.2147/PRBM.S208427.
Gholamzadeh S, Khastavaneh M, Khademian Z, Ghadakpour S The effects of empathy skills training on nursing students’ empathy and attitudes toward elderly people. BMC Med Educ 2018;18:198. https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12909-018-1297-9.
Haley B, Heo S, Wright P, Barone C, Rettigantid MR, Anders M Effects of Using an Advancing Care Excellence for Seniors Simulation Scenario on Nursing Student Empathy: A Randomized Controlled Trial.Clin Simul Nurs2017;13:511–9. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.ecns.2017.06.003.
Larti N, Ashouri E, Aarabi A The effects of an empathy role-playing program for operating room nursing students in Iran.J Educ Eval Health Prof2018;15:29. https://doiorg.publicaciones.saludcastillayleon.es/10.3352/jeehp.2018.15.29.
Li J, Li X, Gu L, Zhang R, Zhao R, Cai Q, Effects of Simulation-Based Deliberate Practice on Nursing Students’ Communication, Empathy, and Self-Efficacy.Journal of Nursing Education2019;58:681–9. https://doiorg.publicaciones.saludcastillayleon.es/10.3928/01484834-20191120-02.
Yang N, Xiao H, Cao Y, Li S, Yan H, Wang Y Does narrative medicine education improve nursing students’ empathic abilities and academic achievement? A randomised controlled trial.Journal of International Medical Research2018;46:3306–17. https://doiorg.publicaciones.saludcastillayleon.es/10.1177/0300060518781476.
Yu J, Parsons GS, Lancastle D, Tonkin ET, Ganesh S Walking in Their Shoes: The effects of an immersive digital story intervention on empathy in nursing students.Nurs Open2021;8:2813–23. https://doiorg.publicaciones.saludcastillayleon.es/10.1002/nop2.860.
Alhassan M Effect of a 2-day communication skills training on nursing and midwifery students’ empathy: a randomised controlled trial.BMJ Open2019;9:e023666. https://doiorg.publicaciones.saludcastillayleon.es/10.1136/bmjopen-2018-023666.
Xue M, Sun H, Xue J, Zhou J, Qu J, Ji S, Narrative medicine as a teaching strategy for nursing students to developing professionalism, empathy and humanistic caring ability: a randomized controlled trial.BMC Med Educ2023;23:38. https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12909-023-04026-5.
Lee SWH, Teh P-L. Suiting Up to Enhance Empathy Toward Aging: A Randomized Controlled Study.Front Public Health2020;8. https://doiorg.publicaciones.saludcastillayleon.es/10.3389/fpubh.2020.00376.
Levett-Jones T, Cant R, Lapkin S A systematic review of the effectiveness of empathy education for undergraduate nursing students.Nurse Educ Today. 2019; 75:80–94. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.nedt.2019.01.006
Bearman M, Palermo C, Allen LM, Williams B Learning Empathy Through Simulation: A Systematic Literature Review.Simul Healthc. 2015;10(5):308–19. https://doiorg.publicaciones.saludcastillayleon.es/10.1097/sih.0000000000000113
Chua JYX, Ang E, Lau STL, Shorey S Effectiveness of simulation-based interventions at improving empathy among healthcare students: A systematic review and meta-analysis.Nurse Educ Today. 2021; 104:105000. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.nedt.2021.105000
Xue M, Sun H, Xue J, Zhou J, Qu J, Ji S, Bu Y, Liu Y Narrative medicine as a teaching strategy for nursing students to developing professionalism, empathy and humanistic caring ability: a randomized controlled trial. BMC Med Educ [Internet]. 2023 Jan 18 [cited 2023 Apr 05];23(1):38. Available from: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12909-023-04026-5.
Yang N, Xiao H, Cao Y, Li S, Yan H, Wang Y Does narrative medicine education improve nursing students’ empathic abilities and academic achievement? A randomised controlled trial.J Int Med Res. 2018;46(8):3306–3317. https://doiorg.publicaciones.saludcastillayleon.es/10.1177/0300060518781476
Yu J, Parsons GS, Lancastle D, Tonkin ET, Ganesh S Walking in Their Shoes: The effects of an immersive digital story intervention on empathy in nursing students. Nurs Open [Internet]. 2021 Mar 20 [cited 2023 Apr 05];8(5):2813–2823. Available from: https://doiorg.publicaciones.saludcastillayleon.es/10.1002/nop2.860.
Wündrich M, Schwartz C, Feige B, Lemper D, Nissen C, Voderholzer U Empathy training in medical students - a randomized controlled trial.Med Teach. 2017;39(10):1096–1098. https://doiorg.publicaciones.saludcastillayleon.es/10.1080/0142159x.2017.1355451
Lorié Á, Reinero DA, Phillips M, Zhang L, Riess H Culture and nonverbal expressions of empathy in clinical settings: A systematic review.Patient Educ Couns. 2017;100(3):411–424. https://doiorg.publicaciones.saludcastillayleon.es/10.1016/j.pec.2016.09.018
Salters-Pedneault, K The Use of self-report data in psychology [Internet]. Connecticut (USA): Dotdash Meredith; 2020 [updated April 14, 2023; cited May 2023 30]. Available from: https://www.verywellmind.com/definition-of-self-report-425267.
Acknowledgements
We would like to thank cienciaupc.pt from Universidade Católica Portuguesa, for sharing our abstract in his website https://ciencia.ucp.pt/en/studentTheses/the-role-of-training-and-education-for-enhancing-empathy-among-he.
Funding
This work is financially supported by National Funds through FCT – Fundação para a Ciência e a Tecnologia, I.P. under the project UID/04279 - Centro de Investigação Interdisciplinar em Saúde (CIIS).
Author information
Authors and Affiliations
Contributions
CTS- designed the study, collected and processed the data and drafted the manuscript. RTA- collected and processed the data and drafted the manuscript. JB- designed the study, collected and processed the data. PCLopes - revised the final document. FC- designed the study and drafted the manuscript. CR- designed the study, drafted the manuscript and revised the final document.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable to a systematic review.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Schwartzkopf, C.T., Alves, R.T., Lopes, P.C. et al. The role of training and education for enhancing empathy among healthcare students: a systematic review of randomised controlled trials. BMC Med Educ 25, 469 (2025). https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12909-025-07038-5
Received:
Accepted:
Published:
DOI: https://doiorg.publicaciones.saludcastillayleon.es/10.1186/s12909-025-07038-5